
Introduction
US hospitals waste an estimated $25.4 billion annually on unnecessary supply chain spending — roughly 30% of all hospital supply expenditures. That figure doesn't capture the full picture. Drug shortages alone now cost hospitals nearly $900 million per year in labor expenses, more than double what they cost in 2019.
The root of most of this waste isn't shipping delays or warehouse mismanagement. It's demand — specifically, the failure to predict, track, and respond to what supplies are actually needed, when, and where.
This article walks through the most common demand-driven inventory problems in healthcare, explains why they persist even in well-funded systems, and offers a step-by-step process to diagnose and fix them. It also covers when a targeted fix is sufficient versus when a full system overhaul is warranted.
TL;DR
- Demand problems — stockouts, overstocking, expired inventory, and poor location visibility — share the same root causes
- Nearly half of supply chain leaders still rely on spreadsheets, which is why these problems persist
- A four-step fix: audit, root cause classification, targeted solution, and monitored validation
- Single-location gaps warrant targeted fixes; recurring multi-site failures typically need a platform overhaul
What Is Healthcare Inventory Demand Management?
Healthcare inventory demand management is the process of predicting, tracking, and responding to the quantity and timing of medical supplies, medications, and equipment needed across care settings.
Unlike retail, healthcare demand doesn't follow predictable purchase cycles. Inventory levels that were well-calibrated one month can be completely destabilized the next — by a flu surge, a mass casualty event, or a newly launched surgical program.
The drivers are varied and often simultaneous:
- Patient volume fluctuations (seasonal and unpredictable)
- Infectious disease patterns and outbreak events
- New service line launches requiring unfamiliar supply profiles
- Regulatory requirements tied to specific care settings
- Emergency preparedness mandates and stockpiling obligations
Standard inventory approaches — static par levels, periodic manual counts, gut-based reordering — are insufficient for this environment. Effective healthcare demand management requires strategies built around clinical workflows, real-time consumption data, and the ability to adapt when patient needs shift.

Common Demand Problems in Healthcare Inventory
Most healthcare inventory failures aren't random — they follow predictable patterns that repeat across facilities, systems, and supply categories. The five problems below account for the majority of waste, stockouts, and cost overruns seen in healthcare supply chains today.
Stockouts of Critical Supplies
Symptoms: Care delays, emergency purchasing at premium prices, staff hunting for substitutes, patient safety risks.
The clinical impact is measurable. 40% of healthcare staff have cancelled a case due to lack of supplies, and 69% of perioperative staff have delayed a case tracking down missing items.
Likely causes:
- Reorder points set too low and never updated
- No real-time tracking — supply levels are invisible until someone physically counts
- Demand spikes (flu season, surge events) not anticipated in par-level calculations
Overstocking and "Emotional Buying"
Symptoms: Cluttered storage, capital locked in excess inventory, supplies expiring before use.
Healthcare organizations typically carry 20–30% of annual supply spend in inventory at any given time, with carrying costs running another 20–30% of that inventory value annually. For a hospital spending $100 million on supplies, that's $4–9 million per year just to hold excess stock.
The behavioral driver is fear. When shortage risk feels high, procurement managers order defensively. A national survey of 700+ hospital pharmacy managers found that 81% reported hoarding available drug supply as a shortage mitigation strategy. It's a rational individual response — but when every manager does it simultaneously, the collective result is artificial scarcity and cascading cost increases.
Expired Inventory
Symptoms: Regular write-offs of vaccines, medications, or perishable supplies; financial losses with no patient benefit.
Industry-average product expiration runs 8–10% of total supply spend. Best-practice targets are below 1%. For a $100 million supply budget, the gap between average and best-in-class represents $7–9 million annually.
Two factors drive most expiration losses: demand miscalculation and the absence of first-in-first-out (FIFO) rotation. Items ordered during shortage fears become excess inventory once the shortage resolves — then sit until they expire. Without an expiration alert system, no one catches the problem until the write-off hits the ledger.

Demand Variability Without a Response Plan
Symptoms: Inventory levels that function in normal periods collapse during seasonal surges, new service line launches, or emergency events.
COVID-19 exposed the extreme version of this problem: by late March 2020, about one-third of US hospitals reported critically depleted face mask supplies. But the same fragility shows up in lower-stakes situations — flu season, a new orthopedic program, a spike in trauma cases.
The root cause is static par levels: set once, rarely revisited, with no mechanism to adjust for volume or acuity changes. When demand shifts, inventory policy doesn't.
Siloed Inventory Across Locations
Symptoms: One facility is overstocked while another has a shortage of the same item; redundant purchasing across sites.
Without centralized, enterprise-wide inventory visibility, each location operates independently — placing orders without knowing what's available three miles away. The result is simultaneous overstocking and shortages of the same SKU across a single health system.
One leading US health system projected $80 million in savings over 3–5 years from supply chain centralization, largely by eliminating this redundancy.
Why These Demand Problems Persist
Most health systems manage inventory through tools that weren't built for the job. Nearly half of hospital supply chain leaders still rely on spreadsheets for inventory management. EHR modules handle clinical documentation, not supply chain optimization. Disconnected systems mean data exists in silos — inaccessible to the people making procurement decisions.
The compounding effect is predictable. When demand signals are missed, procurement responds reactively — spot purchases outside contract, over-correction orders triggered by stockouts. Over-orders produce excess inventory. Excess inventory expires. Each phase of that cycle compounds the cost of the last.
Those costs add up fast across the supply chain:
- Emergency purchasing drives up unit costs significantly above contract pricing
- Expired stock write-offs eliminate millions in supply budget with no patient benefit
- Staff time lost to manual inventory counts diverts clinical resources — nurses spend up to 60 minutes per shift hunting for supplies
- Care quality gaps emerge when the right supplies aren't available at the point of care

How to Fix Healthcare Inventory Demand Problems: Step-by-Step
Fixing demand problems starts with identifying exactly where the breakdown occurs — otherwise organizations invest in solutions that don't match the actual failure point.
Step 1: Audit Your Demand Data and Identify the Gap
Map current inventory usage against actual patient volume and care events over the past 12 months. Identify where stockouts or overstock consistently occur and which product categories are most affected.
Then determine the nature of the problem:
| Problem Type | Description |
|---|---|
| Data problem | No reliable demand data exists — usage isn't tracked meaningfully |
| Process problem | Data exists but isn't being used to guide purchasing decisions |
| System problem | No platform capable of acting on data in real time |
Each requires a different fix. Conflating them leads to investing in the wrong solution.
Step 2: Classify the Root Cause
Before selecting any solution, confirm which category the demand problem falls into:
- Forecasting failure — No demand prediction process; ordering is gut-based
- Visibility gap — No real-time or enterprise-wide inventory tracking
- Behavioral patterns — Emotional buying, hoarding, siloed ordering by department or location
- External volatility — Supplier disruptions, seasonal spikes, new service lines
A visibility gap and a forecasting gap require different fixes. Confirming the root cause before selecting a solution saves both time and budget.
Step 3: Apply the Right Fix for the Root Cause
For forecasting failures: Introduce demand forecasting using historical usage data, patient census trends, and seasonal benchmarks. Business Solutions Group's demand planning platform uses 280+ algorithms to forecast demand across products, locations, and time horizons, replacing gut-based ordering with data-driven par recommendations.
For visibility gaps: Implement real-time inventory tracking across all locations. Enable inter-facility stock transfers to balance supply without triggering new purchasing. Business Solutions Group's Business Performance Solution pulls data from ERP systems, WMS, and other sources into one reporting platform, giving organizations enterprise-wide visibility in place of disconnected spreadsheets.
For behavioral issues (emotional buying, siloed ordering):
- Establish centralized procurement authority
- Standardize par levels using actual usage data, reviewed quarterly
- Deploy cross-location dashboards that surface available inventory before new orders are placed
For external volatility:
- Build demand buffers for high-risk SKUs (critical medications, surgical supplies)
- Develop supplier diversification strategies before a shortage occurs
- Document shortage response protocols in advance — not in the middle of an event
Step 4: Test, Validate, and Monitor
Run the updated demand management approach through at least one full demand cycle — ideally one quarter — before declaring success.
Key metrics to track:
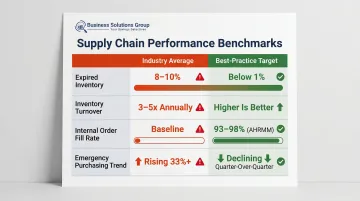
| Metric | Industry Average | Best-Practice Target |
|---|---|---|
| Expired inventory | 8–10% of supply spend | Below 1% |
| Inventory turnover | 3–5x annually (healthcare) | Higher is better |
| Internal order fill rate | — | 93–98% (AHRMM benchmark) |
| Emergency purchasing spend | Trending up 33%+ | Declining quarter-over-quarter |
Establish a regular review cadence — monthly or quarterly — to reassess par levels, update forecasting assumptions, and catch new gaps before they become crises. Organizations that build this review cycle in from the start consistently outperform those that treat demand management as a one-time project.
When to Apply a Targeted Fix vs. When to Overhaul
Not every demand problem requires a full system replacement. Misreading the scale of the problem leads to either under-investment (the problem persists) or over-investment (disruption without proportional benefit).
Apply targeted fixes when:
- The facility is single-location with relatively stable demand patterns
- The core problem is a specific process gap — no expiration alerts, no reorder thresholds
- Incremental improvements like automated alerts and reorder triggers haven't yet been tried
When those incremental fixes have been tried and the problem persists — or when the organization has simply outgrown single-location constraints — a broader overhaul becomes the practical path forward.
Consider a full system overhaul when:
- The organization operates across multiple locations
- Stockouts and overstocking occur simultaneously at different sites
- Emergency purchasing is a recurring budget line item
- The current system cannot produce reliable demand data — at all
At multi-site scale, siloed patches create more complexity than they resolve. Managing disconnected systems across locations generates coordination overhead — duplicate processes, conflicting data, and manual reconciliation — that consistently costs more than consolidating onto a platform built for enterprise-wide visibility. If emergency orders are showing up as a standard budget line, that's the clearest signal the current approach isn't scaling.
Preventive Strategies to Keep Demand Problems From Returning
Demand problems in healthcare inventory aren't one-time events. Without structural prevention, the same failures recycle every season. Three structural changes make a lasting difference:
- Dynamic par levels: Replace static reorder points with demand-responsive thresholds reviewed at least quarterly. Par levels should reflect actual usage trends, upcoming service changes, and seasonal forecasts — not last year's assumptions.
- Proactive procurement: Reactive purchasing — ordering only when stock runs out — tends to cost significantly more than procurement guided by real demand signals. Business Solutions Group's spend intelligence platform supports this shift through consolidated dashboards, real-time analytics, and predictive forecasting, so shortages are caught before they become disruptions.
- Documented processes: Demand problems are often reinforced by informal habits. Established ordering protocols, FIFO practices, and escalation procedures build inventory discipline into daily operations — rather than relying on individual judgment or institutional memory.
Frequently Asked Questions
What are the most common demand-related inventory problems in healthcare?
The most common issues are stockouts of critical supplies, overstocking driven by fear-based ordering rather than usage data, expired inventory from demand miscalculation, and no real-time visibility across locations. Most health systems experience all four simultaneously, to varying degrees.
How does demand forecasting reduce waste in healthcare inventory management?
Accurate forecasting replaces gut-based ordering with data-driven par levels, reducing both excess stock that expires unused and shortfalls that trigger costly emergency purchases. It also makes seasonal demand spikes predictable rather than reactive.
What is "emotional buying" in healthcare procurement and how can it be avoided?
Emotional buying is procurement driven by fear of shortage rather than actual usage data, meaning orders placed "just in case" rather than based on real usage. It's addressed by centralizing purchasing decisions, standardizing par levels, and tying reorder triggers to historical demand data instead of individual judgment.
When should a healthcare facility shift from manual to automated inventory management?
Manual systems become inadequate when stockouts or overstock persist despite process adjustments, when managing more than one location, or when manual counts consistently pull staff time away from patient care. Those are the real triggers — facility size alone isn't the deciding factor.
How can multi-location health systems balance inventory across sites?
Enterprise-wide visibility platforms allow inventory transfers between locations before new purchasing occurs — reducing redundant orders and directing supply to where it's actually needed. This is the mechanism behind projected savings like the $80 million centralization outcome cited earlier.
What role does spend intelligence software play in solving healthcare inventory demand problems?
Spend intelligence tools aggregate purchasing and usage data to identify over-ordering patterns, demand gaps, and cost-saving opportunities. The result is a shift from reactive procurement to a process that catches imbalances before they become crises.


