For businesses, this translates directly to budget pressure. Employer-sponsored family premiums now average $26,993 annually, up 26% since 2020. For healthcare providers and health systems, the pressure shows up in supply chain costs, administrative overhead, and unmanaged vendor contracts.
What's important to understand: these costs rarely become unmanageable through a single unavoidable event. They accumulate through layered inefficiencies — misaligned plan design, fragmented procurement, reactive care patterns, and a persistent lack of visibility into where money is actually going. This article examines all three dimensions of that problem: the decisions that set cost baselines, the management practices that let costs drift, and the systemic context that shapes how costs are generated in the first place.
Key Takeaways
- 90% of U.S. healthcare spending goes toward people with chronic and mental health conditions — making prevention a financial strategy, not just a clinical one
- The biggest savings happen upstream — before costs are set by contracts, plan design, or established care patterns
- Administrative tasks alone represent a $21 billion savings opportunity if fully automated
- Benchmark data is the foundation — organizations that negotiate without it consistently overpay
- Sustained savings depend on continuous monitoring and accountability — not one-time audits
How Healthcare Costs Typically Build Up
Healthcare costs for most organizations don't appear as a single line item. They accumulate across multiple categories: benefits administration, supply procurement, clinical overhead, regulatory compliance, and reactive care spending.
The scale of that dispersion is visible in CMS's own breakdown: hospital care accounts for $1.63 trillion (31% of national health expenditures), physician and clinical services another $1.11 trillion (21%), and retail prescription drugs $467 billion (9%). Those three categories alone represent 61% of all healthcare spending — but each one has its own cost dynamics and requires different intervention strategies.
The Compounding Problem
Cost build-up in healthcare tends to be gradual and largely invisible until scale, audit, or crisis exposes it. A few examples of how this plays out:
- A missed early intervention becomes a high-acuity specialist visit or hospitalization
- An unreviewed vendor contract auto-renews at inflated rates for another three years
- Fragmented purchasing across departments creates duplicate supply orders and excess carrying costs
- Administrative tasks processed manually accumulate hours of unnecessary labor per week
The result: organizations frequently discover they've been managing yesterday's problem with yesterday's data. That gap between what's happening and what's known is exactly where cost reduction starts.
What's Actually Controllable
Some cost drivers are structurally fixed: an aging workforce, rising chronic condition prevalence, clinical complexity. But a substantial portion of healthcare spend is shaped by choices made around procurement policy, plan design, care model selection, and administrative structure.
Organizations that audit these areas — even once — routinely find 10–20% in addressable spend. The strategies in the sections ahead focus on exactly those levers.
Key Cost Drivers in Healthcare
Healthcare costs don't spike randomly — they stem from identifiable, addressable sources. The primary drivers fall into three categories:
Structural drivers:
- Aging population requiring more frequent and complex care
- Chronic disease prevalence — the CDC reports that 90% of the nation's $5.3 trillion in annual healthcare expenditures go toward people with chronic and mental health conditions
- Diabetes alone costs $640 billion annually; obesity nearly $173 billion
Operational drivers:
- Administrative inefficiency — U.S. administrative spending runs between 15–30% of total healthcare spending, compared to roughly 12% in comparable OECD countries
- Fragmented data systems that prevent meaningful cost visibility
- Supply chain waste from unmanaged contracts and non-standardized purchasing
Behavioral drivers:
- Underuse of preventive care that would reduce downstream high-acuity utilization
- Overuse of emergency and specialist services for conditions manageable at lower-cost settings
- Reactive decision-making by both patients and organizations
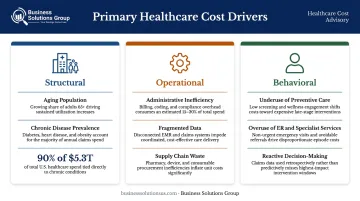
Each category points to a different intervention. For employers managing benefit costs, the dominant problem is plan design misalignment and poor claims visibility — not simply the volume of care employees use. For healthcare providers and health systems, the dominant issues are supply chain inefficiencies, unmanaged vendor contracts, and administrative redundancy. Different stakeholders face different problems, and the strategies that work must reflect that.
Cost-Reduction Strategies for Healthcare
The most effective strategies depend heavily on where in the system an organization operates. A self-funded employer faces different cost levers than a multi-site health system. The strategies below are organized by the mechanism of action — how they actually reduce costs — not just what category they fall under.
Strategies That Reduce Costs by Changing Decisions
These are high-leverage interventions because they shape the baseline from which all downstream costs flow. Getting decisions right upfront is far more efficient than correcting overspend after the fact.
Redesign benefit plan structure to curb unnecessary utilization. Tiered networks and high-deductible plans paired with HSAs reduce premium costs — but only when structured around actual workforce demographics, not applied as a generic template.
Standardize medical supply procurement. Fragmented purchasing and physician preference for higher-cost items without outcome evidence drive significant overspend. Centralizing procurement and benchmarking supplier pricing against market data consistently cuts per-unit costs. Business Solutions Group's spend intelligence capabilities help organizations pinpoint pricing misalignment across their supply categories.
Enforce evidence-based formulary policies. Generic drugs cost 80–85% less than brand-name equivalents, and 773 generic approvals in 2023 alone generated an estimated $18.6 billion in savings within 12 months. Generic substitution, mail-order for chronic conditions, and prior authorization for high-cost drugs reduce spend without affecting outcomes.
Cover preventive care at low or no out-of-pocket cost. Screenings, vaccinations, and chronic disease management reduce downstream high-acuity utilization. Chronic conditions drive 90% of national healthcare expenditures — upstream prevention consistently delivers the highest ROI over a multi-year horizon.
Strategies That Reduce Costs by Changing How Healthcare Is Managed
Most healthcare cost leakage doesn't come from one large mistake — it comes from small, recurring inefficiencies that compound invisibly over time. Improving visibility and control while operations are active closes those gaps.
Use spend intelligence and data analytics to identify cost drivers. Without real-time visibility into claims data, vendor spend, and utilization patterns, organizations manage costs reactively. Analytics tools pinpoint high-cost claims, flag billing anomalies, track contract compliance, and measure wellness program ROI.
Conduct regular claims audits and utilization reviews. Audits catch billing errors, duplicate charges, and out-of-network overcharges common in complex healthcare billing. Utilization reviews surface patterns — repeated high-cost imaging, avoidable ER visits — before they become structural cost drivers.
Negotiate contracts with benchmarked pricing data. Organizations entering negotiations without market benchmarks consistently overpay. Reference-based pricing results make the case: North Carolina's state health plan saved an estimated $300 million per year, Montana saved $48 million over three years, and Oregon's public employee boards saved $112 million in a single year.
Automate administrative workflows to cut transaction costs. The CAQH 2025 Index identifies a $21 billion savings opportunity from automating administrative transactions. A manually processed eligibility verification costs $7.94 and takes 20 minutes; the electronic equivalent costs $2.86 and takes 4 minutes. Multiplied across thousands of weekly transactions, the compounding savings are substantial.

Strategies That Reduce Costs by Changing the Context Around Healthcare
In many cases, the surrounding system — care delivery infrastructure, ecosystem partnerships, access models — is the real cost driver, not the clinical or administrative activity within it.
Expand telehealth and virtual care infrastructure. Replacing high-cost ER visits with virtual consultations cuts the unit cost of routine, low-acuity care. Lower-acuity ED visits average $1,716 versus $178 for urgent care — and telehealth shifts even more of that volume to lower-cost settings.
Build or join integrated care networks. Fragmented care inflates costs through redundant testing, communication failures, and out-of-network billing surprises. Contracting with integrated health systems or building narrow, high-performance networks reduces that exposure.
Address social determinants of health driving avoidable utilization. Housing instability, food insecurity, and transportation barriers contribute directly to preventable hospitalizations. A housing intervention program run by Fallon Health reduced medical spending by $1,352 per member per month — a 38% drop — in the year following intervention.
Optimize the healthcare supply chain for materials and logistics. Health systems managing high volumes of medical supplies and pharmaceuticals face price volatility, last-mile inefficiencies, and contract fragmentation. End-to-end supply chain optimization — carrier contract management, freight cost benchmarking, logistics rationalization — is an often-overlooked lever for large multi-site systems. Business Solutions Group brings carrier benchmarking and logistics expertise to organizations pursuing measurable reductions across their supply operations.
Conclusion
Sustainable healthcare cost reduction starts with understanding where costs actually originate — through clinical decisions, management practices, and systemic structure — then targeting interventions at the source. Organizations that skip the diagnostic step either miss meaningful savings or compromise the quality and access their operations depend on.
This work is also never finished. Contracts expire, populations shift, care delivery models evolve, and new inefficiencies surface. Organizations that build ongoing visibility, governance structures, and expert advisory relationships into their operations turn cost reduction from a one-time project into a durable competitive advantage.
Frequently Asked Questions
Is $200 a month a lot for health insurance?
It depends on the plan type. The average worker contribution for employer-sponsored single coverage is $120/month in 2025 (KFF Employer Health Benefits Survey), making $200 above average for individual plans — but well below the $571/month family average or the $625/month benchmark for unsubsidized marketplace plans. Total out-of-pocket exposure, including deductibles and copays, matters more than the premium alone.
What are the biggest drivers of rising healthcare costs for employers?
The primary drivers are increasing chronic condition prevalence in the workforce, rising prescription drug costs (up 7.2% per employee in 2024), and administrative complexity from fragmented claims management. GLP-1 drugs for weight loss are a fast-emerging pressure point — 66% of large firms now covering them report a "significant" cost impact.
How can businesses reduce employee healthcare benefit costs without cutting coverage?
Plan design optimization — tiered networks, HDHPs paired with HSAs — lowers premiums without reducing coverage quality when matched to workforce demographics. Preventive care investment and claims data analytics then enable targeted interventions rather than broad benefit cuts that erode access without solving the underlying cost drivers.
What role does supply chain optimization play in healthcare cost reduction?
Supply chain spend on medical supplies, pharmaceuticals, and logistics represents a large and frequently unmanaged cost category for health systems. Procurement standardization, contract benchmarking, and freight cost optimization can deliver measurable savings without affecting clinical quality — multi-site health systems frequently uncover substantial pricing gaps once current contracts are benchmarked against market rates.
What are the most common hidden costs in healthcare that organizations overlook?
Administrative waste (duplicate claims, billing errors, manual processing) and surprise out-of-network charges from fragmented care coordination are common but rarely audited. The largest hidden cost, however, is unmanaged chronic conditions — avoidable high-acuity utilization that earlier intervention could have prevented.
How does data analytics help organizations reduce healthcare costs?
Analytics tools give organizations real-time visibility into claims patterns, vendor contract performance, utilization trends, and wellness program ROI. That visibility enables targeted interventions — addressing the actual cost drivers — rather than across-the-board cuts that reduce access without lowering actual spend.